Shoulder Injuries in CrossFit
Introduction
In order to diagnose and direct management of a CrossFit athlete with a shoulder injury, the clinician must have an understanding of typical CrossFit movements. CrossFit include numerous exercises that involve the shoulder joint. Overhead squats, snatches, push presses, thrusters, and push jerks are common movements that place load on the shoulder. The shoulder, not typically a weight-bearing joint, is also used as a weight-bearing joint during gymnastic maneuvers such as handstand pushups and handstand walks. Finally, to the range of motion and power needed for kipping and butterfly pullups and muscle-ups, the shoulder is often stressed and challenged in CrossFit.
This is me doing “JJ”-modified with 135# and Regular HSPU
Additionally, a thorough history, knowledge of the anatomy and physiology of the shoulder complex, and understanding risk factors of shoulder injury are critical in making a correct diagnosis. First let’s look at some basic anatomy.
Basic Anatomy /Physiology
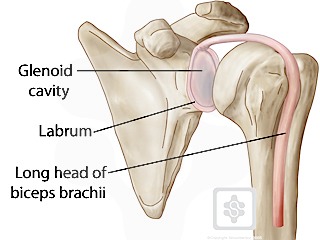
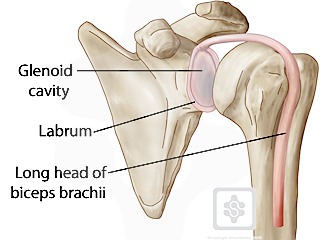
The shoulder is a complex joint consisting of three bony articulations—the acromioclavicular, the sternoclavicular and the glenohumoral joint.
Its complexity is compounded by the biceps tendon and labrum. The long head of the biceps starts outside of the true glenohumeral joint but traverses inside the true joint itself. Adding to the confusion that the “shoulder” to the layperson could mean the back of the neck and trapezius area, make determining the diagnosis of the injury challenging.
Finally layer on top of the joints and articulation all the muscles surrounding the shoulder– including rotator cuff muscles, deltoids, trapezius, serratus anterior, rhomboids, scalenes– and you can see why the diagnosis and subsequent treatment can be complex, even for the astute clinician.
What do the studies say?
While there are limited studies looking at CrossFit injuries and the pattern of injuries, we can learn a lot by delving into the available literature. The studies show that shoulder injuries are common in reported CrossFit injuries, so the clinician taking care of CrossFit athletes should be aware of these movements, the load it places on the shoulder and query the athlete on which movements that causes shoulder pain.
For example, cleans, jerks and snatches are pulling movements that puts high load on the biceps and its attachment into the labrum. Similarly overhead squats can put the shoulder in abduction and external rotation, which also loads the biceps and labrum. In addition gymnastics maneuvers such as handstand push-ups, kipping pull-ups and butterfly pullups can put both eccentric and concentric loads on the biceps. Kipping pull-ups also puts the shoulder in abduction and maximal external rotation, while butterfly pull-ups allows the athlete to quickly cycle pullups using forceful eccentric and concentric contractions of the biceps, lattisimus dorsi and serratus anterior.
Watch Chris Spealler perform and breakdown the butterfly pullup.
Labral Injuries
In the studies out in the literature, there are no studies that look at specific diagnosis of shoulder injuries. Labral tears, with the pull on the biceps and the use of the shoulder as a weight bearing joint, can be a common injury related to CrossFit. The history should ask CrossFitters which movements hurt the shoulder. Anything associated with overhead squats, snatches, thrusters, push presses/jerks should make the clinician consider labral tears in the differential. While the most common shoulder injury overall tends to be rotator cuff tendinopathies, this blog will focus on the labrum. Clinicians should still ensure they do a complete exam.
Diagnosis
Diagnostic shoulder exams for the labrum can be challenging. Common symptoms include anterior shoulder pain, specifically where the biceps tendon enters the joint space and becomes the labrum. Rotator cuff strength is generally preserved. However, the subscapularis, which layers over the biceps tendon and provides stability for the biceps tendon, can be involved with labral tears. Clues to subscapularis involvement is the “lag sign,” where the patient cannot keep the wrist straight while performing a “belly press.” This is also called a “belly press test-modified.” (BJSM)
Special Tests
There are two special tests that are useful for testing the labrum—Speed’s test and the dynamic shear test. While there are many other tests, these are simple and easily done.
Speed’s test
Speeds test is a commonly performed test and if positive, it suggests biceps/labrum involvement. Positive testing includes pain in the bicipital groove area and/or weakness compared to the other side. Speed’s has a likelihood ratio of 2.77 and is more sensitive but less specific and cannot rule in a labral tear, but may help rule it out. (BJSM Hegedus)
Dynamic labral shear test
This test has been described as putting the affected arm at 120 degrees of abduction with maximal external rotation. Then the examiner moves the shoulder from 120 degrees to 60 degrees of abduction while maintaining external rotation. This places shear on the biceps tendon and labrum and may cause pain and or painful click/pops in the anterior or posterior shoulder. (BJSM) I find this test very useful to rule in a labral tear (as it is more specific than sensitive). (Negative Likelihood ratio of 1.54)-BJSM Hegedus.
For the CrossFit athlete, the dynamic labral shear test can be useful test. Thrusters can place shear load on the labrum as the athlete pushes a barbell from a front squat position to overhead with explosive hip extension, forcing the barbell vertical. As the athlete brings the barbell back down to the front squat position, the shoulder position places a dynamic shear on the labrum; similar to the dynamic shear test. Painful clicks and pops during the thruster and similar overhead movements (push press, push jerks) can be a diagnostic clue to labral tears.
Diagnostic injection
If the diagnosis is not clear, but suspicious for a labral pathology, a diagnostic injection of lidocaine into the bicepital sheath at the level of the biceps pulley can help confirm your diagnosis. More than 50-75% relief 10-15 minutes after lidocaine is diagnostic.
Differential Diagnosis-the Acromioclavicular Joint
A key differential is acromioclavicular (AC) pathology, especially in an older athlete. Most have some tenderness over the AC joint and can be simple to differentiate between labrum and AC joint. However, if the diagnosis is not clear, a simple diagnostic and or therapeutic injection into the AC joint can help differentiate pain generating from the AC joint versus labral pathology.
How about the rotator cuff?
While rotator cuff tendinopathy and tears are common shoulder injuries it is not clear if the CrossFit athlete are at increased risk. CrossFit programming with its “constantly varied” movements may help limit the constant focus on the pectoralis minor/major and internal rotation of other recreational weight lifters. Pulling exercises such as rowing, pullups, deadlifts may provide scapular and rhomboid balance which lowers the risk for cuff failure and impingement. Nevertheless, clinicians should keep rotator cuff tendinopathy and tears in the differential but not be surprised if the cuff appears strong and healthy on examination. A subacromial injection may help ascertain diagnosis.
TREATMENT
Rehabilitation
Any patient who has a shoulder injury should be started in a physical therapy program for rehabilitation even if the labrum is considered the primary disorder. Ideally this should be a therapist with familiarity with CrossFit movements and how to return the CrossFit athlete back to CrossFit. The therapy should focus on strengthening of the dynamic stabilizers of the shoulder, the rotator cuff and the scapular stabilizers. Proprioceptive exercises can also facilitate return to sport and should be included in the rehabilitation. Sleeper stretches can also help with posterior capsule tightness and mobility issues.
Modifications
Strengthening of the dynamic stabilizers of the shoulder, specifically the external rotators should be emphasized and can be continued during warm ups or cool downs using light resistance bands. All overhead movements should be pain-free. If pain free without load, the clinician can encourage the athlete to work on mechanics and consistency of technique and limit the load to pain free loads. Working on movement with the PVC pipe or light weight can keep the athlete active and engaged. Other pulling movements, such as rowing, light deadlifts, and ring rows can help strengthen the scapular stabilizers and should be encouraged if pain free. Shoulder proprioception exercises such as those emphasized in the “Turkish Get-ups” may help improve core stability and shoulder stability. Russian kettlebell swings can also be included as long as the athlete remains pain free during the range of motion. Athletes should be encouraged to work on front and back squats, box jumps, and even running.
Keeping the athlete and modifying the WODs can keep the athlete an active participant in their rehabilitation.
Follow up
After 6-12 weeks of modification of exercise and rehabilitation, the athlete should be re-assessed for any improvement in pain. If the athlete continues to complain about pain with overhead movements, then continued evaluation to ensure the diagnosis is correct is warranted. An MRI is useful but may need contrast to see labral injuries and its use should be considered judiciously and always be used in conjunction with your clinical suspicion. Further modification of exercises with continued rehabilitation may be considered if the athlete is making improvement.
Surgical Options
Finally, surgical consultation may help give the athlete full options in returning back into CrossFit. A labral tear will generally not heal, but the body may modulate the pain response where people can return to doing most activities. There is a paucity of literature available on long term effects of labral tears but if the patient is adverse to surgical options, many may be able to continue to modify activities while still performing most CrossFit WODs without surgical intervention. The athlete who has failed conservative measures and is looking to return back to high level CrossFit should be referred for surgical considerations. Here again, diagnostic injections into the bicepital groove may help surgeons identify the pain generator. Surgical options include labral repair with or without biceps tenodesis. Finally, the athlete should be aware that surgery will generally involve 4-6 months of rehabilitation for full recovery.
REFERENCES
Myer CA, Hegedus EJ, Tarara DT, et al. A user’s guide to performance of the best shoulder physical examination tests. Br J Sports Med 2013;47:903–907. PMID: 23322891
Hegedus et al. Which physical examination tests provide clinicians with the most value when examining the shoulder? Update of a systematic review with meta-analysis of individual tests. PMID: 22773322
http://bjsm.bmj.com/content/46/14/964.full.html


Reblogged this on Dr. Robert Oh, MD.
LikeLike
hey doc, i just saw this post. i hope you could get back to me. i love sports and kind of sports, i love lifting anything, i love doing high intensity workouts, i love doing things that requires lifting, workouts that are not stagnant i hope you know what i mean. but the problem is i am always on the hold in doing stuffs that i love to do. you see, since i heard and watch high intensity workout i love doing it no doubt about it. then i tried conventional gyms but it didn’t work out for me cause i hate routines and long waits for reps and stuffs. since i learned, heard and watched crossfit (actually i didn’t know that it was crossfit before) i told myself i want that, i would love to give that a try but like what i said i am always on hold in doing it because the problem is i have a shoulder injury, i dislocated my right shoulder several times already before of basketball varsity and volleyball varsity. my doctor recommended me to surgery of my shoulder which is implanting it with tacs to hold my shoulder i know you know this. but i haven’t done that yet (financial problems). the question is should i go and try crossfit or just have my surgery first and rehab then do crossfit cause all my life i’ve been fit and well but after my dislocations and injury i lost it all. please help me. i really wanted to get back on track of my fitness. im longing for help. thank you.
LikeLike
Sounds like you have instability of your shoulders. Whether you have mutidirectional or traumatic or both, in either case, you should give rehab a try. This is working on your dynamic stabilizers of your shoulders (rotator cuff, scapular stabilizers) and also on proprioception. If this does not work you can always do surgery. So my recommendation is undergo rehab, then give CrossFit a try. You can also do rehab while doing CrossFit, but you’ll have to find a place and coaches that really understand the shoulder and the scaling you will have to do at first. CrossFit has lots of overhead arm activity, and those with instability without strength may dislocate during some movements.
LikeLike
thank you very much for having the time to respond to may mail. well, my doctor here told me that i should have my surgery but we don’t have yet the money. but thank you.
LikeLike
Dr. Oh,
I am a physical therapist currently undergoing an orthopedic residency program. I have a big presentation coming up, where we are expected to present something “new” to the residency faculty members. Being a crossfitter myself, I want to present on proper diagnosis and treatment of shoulder injuries in crossfit athletes and the sports comprising crossfit (weight lifting, oly lifting, gymnastics, etc.). I would love to discuss this topic more with you. Please contact me at your convenience. Looking forward to hearing from you.
Sincerely,
Meaghan Dayton PT, DPT, CSCS
LikeLiked by 1 person
Let’s talk! Would love to chat. thanks for the comment.
LikeLike
Thank you doctor for writing this post.
I have been CrossFitting for nearly 4 years now. I would do all movements and lifts. About 5 weeks ago, I dislocated my right shoulder from a snowboarding accident (I am right hand dominant). Since I was on a mountain, my arm wasn’t reduced for another 5 hours.
After reduction, I did not have sensation on my deltoid. I was able to move and have feeling from my biceps to my fingers, but nothing in the deltoid. I started receiving sensation (while slowly) over the past few weeks. About 10 days ago I was finally able to lift my right arm under my own strength.
I have been rehabilitating via PT for the past 5 weeks. My PROM is pretty mostly all there, but the AROM is not as good. Sensation is returning in my shoulder, but it still not at 100%. I can lift my arm above my shoulder but it takes a great deal of concentration and strength in order to do so.
My question is this: I want to go back to being an avid CrossFitter. I am wondering if it is better for me to have surgery to repair my large tear involving the anterior and inferior aspects of the glenoid labrum and adjacent cartilage. Tear at the insertion of joint capsule to the inferior aspect of the glenoid and a high-grade partial-thickness articular sided tear of the distal supraspinatus tendon (the only tears according to my MRI report), or is it better for me to keep up with PT and eventually heal. I want to go back to doing kipping pull-ups, HSPUs, muscle-ups, snatches, etc. My PT is saying that if I have the surgery, that I will not be able to do those actions anymore.
I understand that if I do have the surgery, that I will be in a sling for 4-6 weeks, and out of commission for a total of 4-6 months. I am able to deal with that. What I can not put up with is not being able to do the things I’d like to do. I do not want to live with having restrictions. And that does not just mean CrossFitting. I’d like to swim, play baseball, basically live life without any restrictions.
What would you recommend?
Thank you in advance,
Juan
LikeLike
More P.T. won’t hurt. However, that being said, labral tears don’t heal..P.T. can modulate the response to pain by building up the dynamic stabilizers of the joint and your body can potentially recover to pain free movements. Again, though, if you are wanting to go to high level CrossFit, with all those movements, then I would consider surgery if your pain/function does not improve after p.t. I am not sure if what your pt says is true–I know many cross fitters with labral tears and they are back to dong all those movements after surgery and rehab. Hope that helps?
LikeLike
I completely agree with Dr. Oh. With that large of a tear involving the labrum and Rotator Cuff, surgery is needed to attain the stability you need to do the activities you love. And yes, you can get full mobility and strength back after surgery with proper rehab. Find a PT who is familiar with Crossfit and is dedicated to getting you back from the beginning of the process. Keep doing rehab before surgery, you want as much ROM and strength as possible to make rehab after surgery easier. Good luck!
LikeLike
Hi there I am an avid Cross-Fitter and PT. I have just had surgery for a 2cm full thickness cuff tear and bicep tenodesis for a grade II SLAP lesion plus subachromial decompression. The other shoulder will need surgery too although the pathology shows it’s not as bad. I was wondering if it’s better to have the other shoulder done sooner – within 6 months – so that I can rehab them both together, or wait a year to get full strength back to my first shoulder? Also what is the likelihood of me being able to do all the Cross-Fit moves again? I would love to get back to at least small team comps. I’m 48
Thanks
LikeLike
Hi Annabel. this is of course athlete’s preference, but if it was me, I’d do it one shoulder at a time, see how functional and how happy I am with shoulder #1. You should be able to get back to full crossfit, but you may find your limitations in your surgical shoulder vs. your other shoulder as you gain back your strength and mobility. Good luck!!
LikeLike
Hi Annabel I just read your post and am just about to have bicep tendonesis surgery. We are about the same age and I am also an avid crossfitter. I was wondering how your surgery and rehab went.? I have made the decision to have both shoulders done straight after one another I travel a lot and just don’t see how I can be out of action for so long so no choice really, I hope it works out as I also want to carry on competing!
LikeLike
So the surgery went well but I needed about a year between getting each shoulder done as the rehab takes a while and the first shoulder will need to be strong and capable to do everything while the second shoulder is in a sling (6 weeks) Since the surgery my shoulders have been much better but they can’t tolerate too much. I believe this is more because the mobility I lacked is still there so it is worth addressing the issues that caused them to tear in the first place. Hope that helps and good luck!
LikeLike
Thanks so much!
LikeLike
Hey Doc, after an MRI I was diagnosed with a full labral tear in my left shoulder last year, an injury likely caused by playing competitive golf for almost 20 years. I have always been extremely active both inside and outside of the gym, doing strength training 5-6 days per week on average, but was only experiencing pain during the golf swing. Both surgeons I met with were unable to recreate the pain in my shoulder so they recommended I do band work to strengthen the shoulder stabilizers and rotator cuff, so I’ve done the band exercises 3X per week for the past year and the pain has disappeared completely. I am now interested in trying CrossFit for the first time, but want to proceed with caution! Do you have any specific words of wisdom or advice? THANK YOU!
LikeLike
Hi Jeff. Sounds good. CrossFit has a lot of overhead movements and lots of pulling and pushing (i.e pull-ups, cleans, jerks, thrusters etc). These can pull/put load on the biceps/labrum complex but if you have rehabilitated the shoulder, as long as you go slow and feel stable overhead, you should be ok. just ensure you tell the coaches and don’t be afraid to scale a lot until you have better form. In CrossFit -it’s about technique/form and then once you are consistent with form/technique, then you can dial up the intensity. Also — listen to your body!
I had a pain in my shoulder, i dialed down the weight overhead (really felt it during thrusters) an continued to work on form and then magically–in about 7 months, I was fine!
LikeLike
One more question: Are there any specific movements you would recommend I avoid entirely? Muscle ups, kipping pull ups, handstand push-ups, etc? These seem like they could put a lot of strain on the shoulder…
Thanks!
LikeLike
I would agree with those — but that doesn’t mean you won’t be doing them with time and strength. lots of substitution — strict pull ups and negative pushups, strict dumbbell presses and strict shoulder presses helps build strength first . then once you feel stronger, adding hollow rocks and working on the movement would be good to start.
LikeLike
Awesome, thanks for the advice. SUPER helpful, I really appreciate it!
LikeLike